

Your Top Dental Implant Questions Answered by Our Doctors
If you’re researching dental implants, you’ve probably realized by now that there is a lot of information out there. There are different terms, contradictory opinions, and dentists who may have even told you that you aren’t a candidate. We hear this every single day, and more often than not, that is not the case.
We recently sat down to answer some frequently asked questions submitted by members of our dental implant community, and we’re turning those answers into this guide so you have something to come back to.
In this guide, we cover:
- Who is a candidate for dental implants?
- Zygomatic vs. pterygoid vs. short implants vs. bone grafting — what’s the difference?
- What customization options are available?
- What are the sedation options for implant surgery?
- Are dental implants better than dentures?
- What is bone grafting and do I need it?
Who Is a Candidate for Dental Implants?
Short answer: almost everyone.
The list of conditions that would genuinely prevent someone from getting dental implants is very short, we’re talking about a handful of cases per year. The primary contraindications are a history of radiation to the jaw, very poorly controlled diabetes, and certain bone cancer medications. Even then, there are often workarounds. We’ve successfully placed implants in patients with radiation histories by consulting with their oncology team to identify safe zones, and in some cases using hyperbaric chamber therapy to improve bone vascularity beforehand.
The bottom line? If you’ve been told you’re not a candidate, please get a second opinion. We see patients almost every day who were turned away elsewhere and are absolutely candidates for implants. You’re very likely one of them!
Zygomatic vs. Pterygoid vs. Short Implants vs. Bone Grafting — What’s the Difference?
This is one of the more technical questions we get, and it’s worth breaking down clearly.
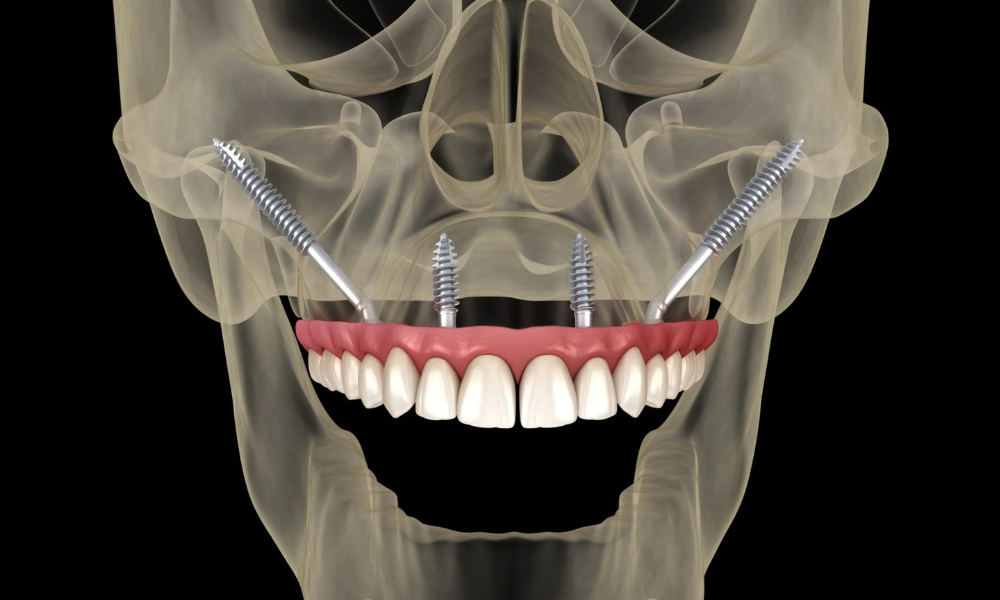
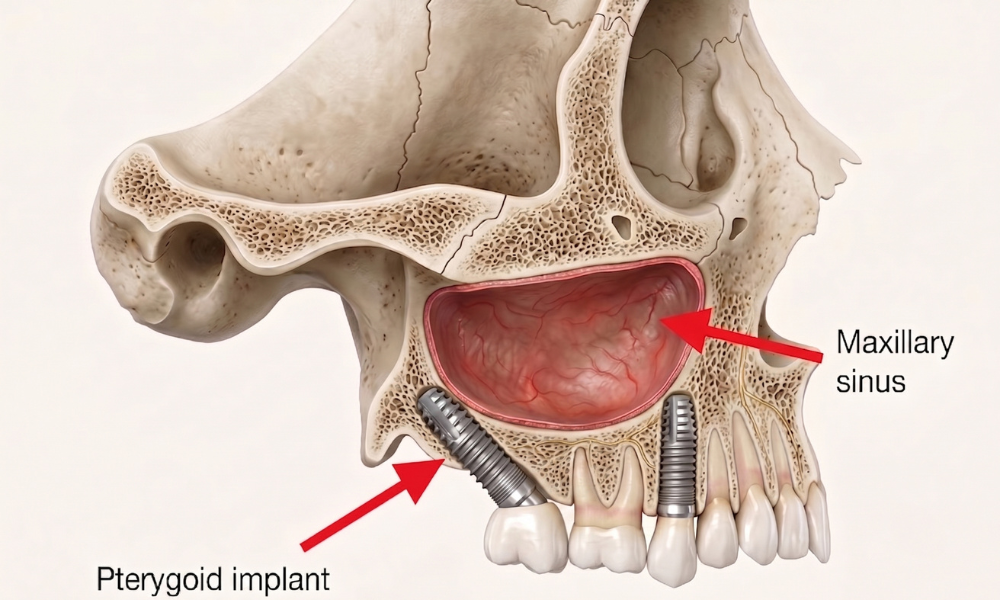
Pterygoid implants are the most commonly needed alternative to a standard All-on-4. They’re placed in the bone behind your sinus, providing a rear anchor point when your sinus extends further forward than average. Think of it like a glass tabletop, if it’s fully supported, it holds up fine. However, if it hangs off the edge, it’ll snap. Pterygoid implants eliminate that “cantilever” by giving your restoration a solid back anchor.
So when a patient has a larger than average sinus, rather than leaving unsupported teeth in the back, we add a pterygoid implant where there’s dense bone behind the sinus. The good news is that pterygoid and zygomatic bone behave more like arm bone than jaw bone, so it doesn’t resorb the way alveolar bone does, so nearly everyone has enough of it to work with.
Zygomatic implants go into the cheekbone and are used when there’s very little alveolar bone remaining. They’re effective, but here’s what we need to say plainly: they are criminally overprescribed. We do a high volume of implant cases, and zygomatic implants come up maybe once a month. We’ve had patients travel from other states after being told they needed zygomatics, and they didn’t. The procedure is more involved, more costly, has a longer recovery, and carries additional risks like sinusitis and soft tissue complications. If you’ve been told you need zygomatic implants, don’t panic, just get another opinion first.
Our overall philosophy: always plan for the next step. If traditional implants can work now, that preserves zygomatic implants as a future option if ever needed. Going straight to zygomatics leaves nothing in reserve.
Short implants are primarily used in the lower jaw (mandible) when there’s limited bone height above the inferior alveolar nerve. They work very well in the right situation and are a far simpler solution than more aggressive approaches.
What Customization Options Are Available?
More than most people expect!
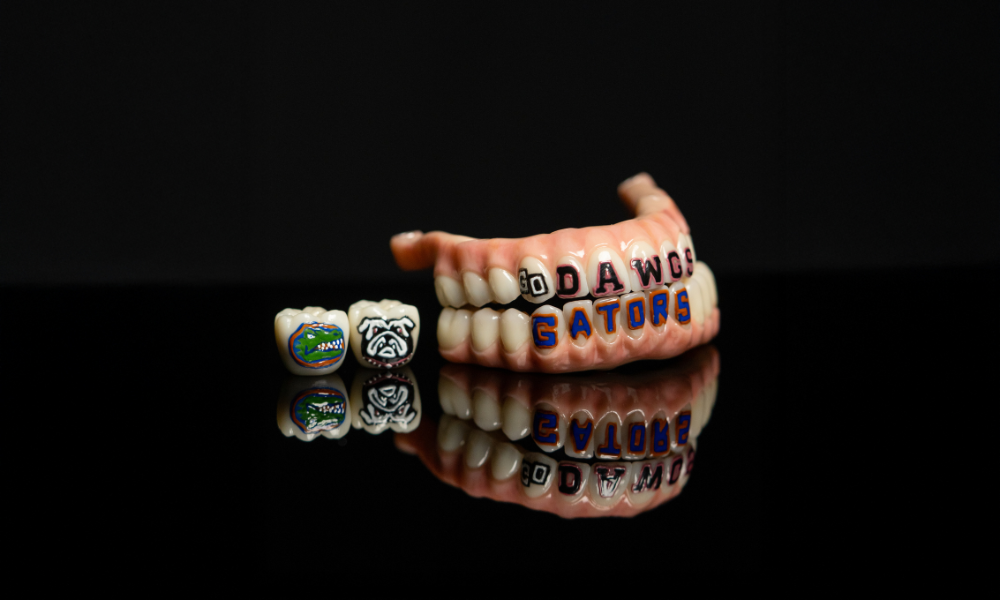
The teeth that sit on top of your implants are fully custom-designed. We start by taking 3D scans of your face and teeth to design proportions that are specific to the size and shape of your face. From there, everything is on the table.
Want sharper canines? Done. A gap between your front teeth? Easy. A more natural, slightly “lived-in” look with realistic staining? Absolutely. Want to match a celebrity’s smile? We can do that too.
We’ve also done tooth tattoos (including a David Bowie lightning bolt and a Miami U logo), diamonds, and even a full gold front tooth paired with zirconia everywhere else. If you want it, we can make it, because everything here is milled and finished custom, in-house.






What Are the Sedation Options for Implant Surgery?
About 95% of our surgeries are done with some form of sedation, and for good reason, you shouldn’t have to white-knuckle your way through a major dental procedure.
Our most common option is oral sedation, which is highly effective and leaves most patients with little to no memory of the procedure. For patients with higher anxiety or more complex cases, we offer IV sedation administered by a board-certified anesthesiologist, not an assistant, not a CRNA. This is hospital-level anesthesia in our office, and it’s about as safe as it gets.
We also keep the environment as comfortable as possible: lights dimmed, your music playing, familiar faces. If you need anesthesia, there is zero shame in that. We would choose sedation for ourselves.
Are Dental Implants Better Than Dentures?
Yes. Unequivocally.
Implants look better, feel better, function better, and last longer. They don’t come in and out. They don’t slip. You can eat whatever you want. There’s no rubbing or irritation. The only category where dentures “win” is upfront cost.
The quality-of-life difference between full implants and dentures is hard to overstate. It’s less like comparing two dental solutions and more like comparing driving somewhere versus walking. Sure, both get you there, but they are not remotely the same experience.
What Is Bone Grafting and Do I Need It?
Bone grafting is used to either preserve existing bone or rebuild bone that’s been lost over time.
When a tooth is extracted, the surrounding bone begins to shrink, studies show it can lose 70–80% of its volume in the first year alone. A bone graft fills that socket after extraction, minimizing shrinkage and keeping the site viable for an implant down the road.
For patients who lost teeth years ago, significant bone loss has likely already occurred. In those cases, grafting rebuilds the ridge before we place implants, taking a site that might only have 2–3mm of bone and growing it to 6–8mm, which is what we need for a stable implant.
We sometimes add grafting even when it wasn’t in the original treatment plan, because we’d rather do it right once than have a patient return years later without enough bone for a replacement implant. It’s always about setting you up for long-term success.
Ready to Find Out If You’re a Candidate for Dental Implants?
Whether you’ve been turned away before, you’re just starting to research your options, or you have questions that weren’t covered here, we’d love to talk. The best place to start is a complimentary consultation, where we can take a look at your specific situation and give you a real answer. If you don’t live in or near Jacksonville, FL, we also offer virtual consultations.
You can schedule online here, or click the button below to give us a call.
Watch the full video version of this Q&A on our YouTube channel, and join our dental implant community group on Facebook!


